Shock to the System, a new breed of injury?

news.omega
..."His own theory pinpoints electromagnetic pulses as one possible culprit. Blasts emit intense magnetic fields that may damage brain cells, he contends."...
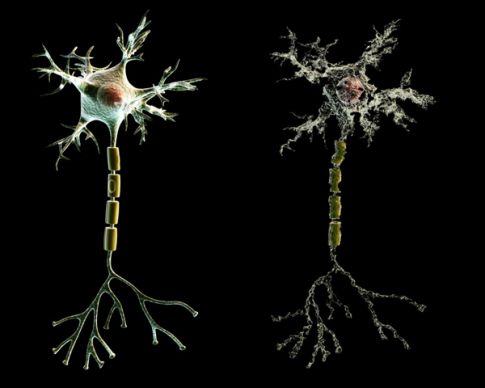
Photo by Medi-Mation
Shock to the System
Soldiers who manage to walk away from explosions in Iraq may actually be suffering terrible—yet invisible—brain trauma. Could blast waves be fueling a new breed of injury?
By Eric Hagerman Posted 08.22.2008
http://www.popsci.com/military-aviation-%2526-space/article/2008-08/shock-system#
August 15, 2008— The first time Army Specialist Frederick Hussey “got blown up in Iraq,” as he says, was on Easter Sunday, April 16, 2006. Hussey was five months into his yearlong deployment as an infantry medic when a cluster of anti-tank explosives jolted his Humvee off the road some 50 miles south of Baghdad. The blast filled the cabin with acrid black smoke, but Hussey was able to jerk the wheel back and steer the truck to safety. “Everybody ended up being OK with that one,” Hussey says. “You know—shook up and all, but there was no loss of life. I would say that one just rang my bell really hard.”
Hussey stands a sturdy 5-foot-10, speaks with a Southern twang, and prides himself on being the only guy the other guys will hug—the papa bear to his fellow cavalry scouts. He worked for 13 years as a grocery-store manager after returning from the Gulf War, and then in 2004 he reenlisted, asking to be a medic because he wanted to help.
The second, third and fourth times Hussey was hit, he was riding in vehicles when they were destroyed by improvised explosive devices, or IEDs, buried in the road. During one attack, he took shrapnel to the cheek and was briefly knocked out. Another one earned him a patch that reads “IED bait” from his buddies. But each time he managed to walk away.
Number five was the worst. He and six others from his platoon were patrolling on foot near their base when an IED blew everyone off the road. “The last thing I remember was seeing my feet in the sky,” Hussey says. “I could hear them hollering for a medic, so I got up, but I kept falling over. I think that’s where my headaches and my hearing damage came from.” He was back on patrol inside of a week.
Hussey was “functioning at about 75 percent,” he says, when two weeks later a rocket-propelled grenade delivered his final blast of the war, exploding against a cement wall 20 yards away as he tried to hustle an injured soldier to safety. It knocked him down but didn’t knock him out—another close call.
Or so he thought. Within a year of his return home, Hussey was told he had post-traumatic stress disorder (PTSD), a psychological condition that can develop in the emotional aftermath of a life-threatening event. He was also diagnosed with a mild traumatic brain injury, the medical term for concussion. Only there’s nothing mild about it. His experience left him with constant headaches, nausea, garbled hearing, insomnia and alarming memory lapses. Concussion symptoms are supposed to clear up in a few weeks or months, but two years later, Hussey, 39, still has them. “At first I thought I was doing OK,” says Hussey, who is now posted at Fort Jackson, in his hometown of Columbia, South Carolina. “But as time went by, it got to where I couldn’t remember the names of guys I was deployed with. I was having difficulty concentrating. It started snowballing, and I was forgetting things and struggling to cope. It’s hard to explain, but it’s just affected everything I do.”
Thousands of American soldiers are coming home with similar complaints. The big mystery is why. Plenty of them have been hit in the head like Hussey, but even those who haven’t are turning up with unusually protracted symptoms that resemble those of a serious brain injury. One tantalizing clue is that among the 2,500 soldiers who returned from yearlong tours in 2006, 62 percent reported that they had been exposed to two or more explosions, whereas only 2 percent had suffered gunshot wounds. The trend has researchers wondering: Is there some unaccounted-for mechanism in the blast itself that’s causing hidden brain injuries?
Neuroscientist Ibolja Cernak, a medical director at Johns Hopkins University’s Applied Physics Laboratory, is one of a handful of researchers across the country trying to find out. She believes that blasts may do more than just rattle the head; the shock waves also compress the torso, which may cause pressure waves to ripple through blood vessels like miniature tsunamis, rushing into the brain and damaging tissue. Army Colonel Geoffrey Ling, a neurologist who has treated troops in both Afghanistan and Iraq, agrees that there’s probably more to war-zone head trauma than the blunt forces at play in a car accident or football collision [see “Gridiron Gear Goes to War,” page 86]. His own theory pinpoints electromagnetic pulses as one possible culprit. Blasts emit intense magnetic fields that may damage brain cells, he contends. “People are seeing a syndrome among these returning veterans,” Ling says. “The question I have is, what’s causing it? If I know the answer to that, potentially I can prevent it.”
With 178,000 soldiers deployed in Iraq and Afghanistan, and thousands more gearing up for second, third and sometimes fourth tours of duty, these questions have sparked a surge in funding. Late last year, Congress earmarked $300 million for basic science research on brain injuries and PTSD. The National Institutes of Neurological Disorders and Stroke recently called together more than 100 doctors, neuroscientists, physicists and biomechanical engineers to review the little that is known about blast-related brain injuries. And the Defense Advanced Research Projects Agency, or Darpa, is in the midst of a yearlong, $9-million effort, led by Ling, to study the effects of blasts on the brain—from chemical and structural alterations to, ultimately, behavioral symptoms.
Meanwhile, soldiers and their doctors are waiting for answers to rudimentary questions about diagnosis and treatment. Above all, what everyone really wants to know is whether blast exposure—with or without direct damage to the head—triggers long-term neurological problems that are waiting to ambush an entire population of veterans.
A Hidden Danger
Some 97 percent of American troops wounded in Iraq come home alive. The survival rate is higher than in any other war, and is largely thanks to improvements in body armor, evacuation procedures and medical care. The Kevlar vests and helmets worn by today’s combat troops, for instance, have saved soldiers who may have otherwise died from bullets and shrapnel. The catch is that more of those soldiers are coming home with permanent injuries from explosions than ever before.
There are many ways to be wounded in a blast. The detonation turns the bomb material into pressurized gases that expand instantly, radiating a supersonic wall of air many times as powerful as hurricane-force winds. That primary blast wave leaves a vacuum in its wake, and the pressure differential creates shearing forces that cause organs to expand and then collapse, crushing lungs and bursting eardrums. Shrapnel and debris can cause further damage, and there is always the chance of getting burned by the heat or slammed into something.
What nobody knows is what all these forces do to the brain. A blow to the head from a blunt object can cause a concussion, certainly, but how is it that soldiers are coming home with brain injuries without ever having been hit in the head? A military task force acknowledged in April that the rate of traumatic brain injury “is thought to be significantly higher than in any previous war.” In a report called “Invisible Wounds,” the public-policy think tank the Rand Corporation estimated that as many as 19.5 percent of soldiers—320,000 of the 1.64 million soldiers sent to Iraq and Afghanistan—may suffer from traumatic brain injury. It’s impossible to say how many of them have actual damage, though, because a diagnosis would require more tests, and 57 percent of the people in this group report that they have never undergone medical evaluations for head trauma. “We have one in five soldiers with a probable traumatic brain injury, and we just don’t know what that means in terms of future impairments and needs,” says Terri Tanielian, a Rand senior research analyst who edited the report. “The unknown really is the public-health concern.”
Part of the difficulty facing researchers and doctors is that the military’s concusssion-screening questionnaire asks soldiers to report events they may well have forgotten. Even in the hospital, symptoms of mild traumatic brain injuries are easy to miss because the subtle bruising or swelling rarely shows up on scans, and in many cases there may be no gaping wound to call attention to the problem in the first place. So doctors are left to work backward from symptoms: A soldier with a traumatic brain injury might complain of headaches, sleep disturbances, and sensitivity to light and noise, and neuropsychological testing may reveal cognitive sluggishness. Not surprisingly, these changes can make people irritable and transform their overall personality, jeopardizing their relationships and jobs. “They come home a different person,” says Hussey’s doctor, Steven Scott, who runs the brain-injury clinic at the James A. Haley Veterans Hospital in Tampa, Florida. “Almost everyone is willing to accept that there’s an emotional component, but they don’t feel that’s the only explanation. When you look at the power of these blasts, it makes so much sense.”
Confounding the diagnosis in blast victims is the overlap with PTSD. It’s possible that a violent explosion could cause both physical and psychological trauma. “We do the best we can to try to sort them out,” says neurologist Gary Abrams, who heads the rehabilitation center at the San Francisco Veterans Administration Hospital, “but it’s very difficult.”
As a result, soldiers with undocumented brain injuries may never get the right medical benefits and care. The military is wrestling with how to determine whether soldiers who seem fine after surviving an explosion should return to combat. After all, if every IED victim were evacuated, the loss would gut the military’s fighting capability. And from a tactical standpoint, the military needs to know what’s causing these injuries before it can design better gear to protect soldiers.
Aftershocks
Specialist Hussey keeps a hectic schedule these days. He and his wife are separated, and he takes care of his two teenage sons in a small apartment close to Fort Jackson. Aside from his duties as a single father, his weekly roster of appointments includes 15 to 20 clinical visits—to a neurologist, psychologist, psychiatrist, occupational therapist, physical therapist and pain specialist, as well as PTSD and Alcoholics Anonymous group meetings. The passenger seat in his car used to be littered with appointment slips before the Army issued him a PDA to keep track of it all, as it has started doing with brain-trauma patients.
Probably because his symptoms are so broad, it took a while for Hussey to realize that there might be something wrong beyond the PTSD and physical wounds. It was about five months after he returned from Iraq that he first began to notice mental lapses. He and a fellow medic were catching up, and his buddy mentioned a story about the day they met at a patrol base south of Baghdad in 2006. A mortar had landed inside the compound, and instead of hitting the deck, the Iraqi soldiers with them had fled. “It was kinda comical when it happened,” Hussey says. “It was like throwing a wolf into a chicken coop. Those guys just took off. They were running outside the damn patrol base!” But when his friend told the story, Hussey didn’t laugh. He was alarmed, because at first he couldn’t recall it ever having happened. “He kept trying to convince me and remind me, but I just had absolutely no recollection whatsoever,” Hussey says. They went over and over the incident until Hussey eventually pieced together the memory.
Not until Hussey joined an AA program at a Veterans Administration mental-health clinic a year after he returned did he discoverer that he had a brain injury. A nurse who gave him a routine screening test for mild traumatic brain injury—standard for patients at the clinic—diagnosed him on the spot. A doctor at the clinic confirmed the diagnosis, and Hussey was sent to the brain-injury center in Tampa, where he spent two weeks undergoing a battery of tests: brain scans, psychiatric evaluations, EEGs. That’s when he met Scott, who mapped out a rehabilitation program for Hussey. Mostly it includes managing symptoms such as chronic pain, headaches and insomnia, and offering ways to organize his life.
Aside from the PDA, Hussey’s strategy for dealing with his spotty memory is low-tech. “You just make a list and try to get into a routine,” he says. “There’s a certain way I drink out of my coffee mug, a certain way I turn the lid. I am routine to hell and back.” The repetition strengthens his memory.
His lasting physical wounds include a broken nub of bone and cartilage at the base of his sternum, a scar under his eye from shrapnel, a cracked cervical vertebra that sporadically numbs his arms down to the elbow, and nerve damage in his eye that his neurologist blames for the headaches.
Hussey’s case is complicated—but far from unique—and those are the challenges military doctors face in diagnosing battle-related brain injuries. Perhaps even more challenging is pinpointing how the damage happens in the first place.
The Blood-Wave Theory
Scientists have been studying blast waves since the dawn of ballistics, but they have never really looked at what pressure waves do to the brain. The conventional military wisdom is that although the eardrums, lungs and bowels are vulnerable to bursting, the brain—protected as it is by the skull and helmet—is relatively immune.
Not true, says Johns Hopkins’s Cernak, who worked as a doctor and researcher at a military hospital in Belgrade from 1986 to 2001 during the Yugoslav wars. When I visit her at her office, she looks formal in her gabardine suit, but her manner is warm (her colleagues call her “Ibi”). Trying to match her brisk stride, it’s not hard to picture her on the battlefield collecting blood samples from soldiers, as she did in Belgrade. That’s when she first noticed soldiers with unexplained brain injuries.
Cernak conducted a series of intensive tests on 1,300 soldiers who had survived an explosion with extremity wounds but no visible head trauma. She found that half of the soldiers had internal blast injuries that would have been missed without close inspection. But what really caught her attention was that a surprising number of this group complained of neuropsychiatric symptoms such as vertigo, headaches, nausea, dizziness, nightmares, and lapses in memory and concentration.
Blood tests revealed that many had altered brain-hormone levels, and EEG tests showed that 36 percent of the blast-injured group had abnormal brain-wave activity, as did 12 percent of the group with only extremity wounds. When Cernak’s team re-administered a battery of neurological and psychological tests up to a year later, 30 percent of the injured group still showed neurological damage, along with 4 percent of the other group. In other words, she found signs of long-term physiological changes in the brains of soldiers who never suffered head wounds. “The major point is that these people did not show improvement, even after one year,” Cernak says. “The implication is that even the slightest damage due to a blast may go together with brain dysfunction. But what is the mechanism if the person didn’t get hit on the head?”
Ever since her pioneering study, Cernak has been trying to prove her theory that blast waves indirectly damage the brain, and to figure out how. She is now the medical director of the national-security technology department at Johns Hopkins University’s Applied Physics Laboratory. She spends much of her time working with the engineers in the APL’s Impact Biomechanics Test Facility, which houses a hydraulic impact sled for testing car seats and a 60-foot-long steel pipe called a shock tube that simulates the force of a blast wave.
From the protection of the impact lab’s control room, one of Cernak’s colleagues punches in a computer command to fill a chamber at one end of the shock tube with compressed air and then fire it down the tube at 760 miles per hour. Today’s target is a pink plastic torso complete with synthetic organs and dozens of pressure and acceleration sensors to measure the impact of the blast. But Cernak’s usual mark is a rodent.
In one of her most cited studies, Cernak compared the brains of rats whose entire bodies were exposed to the blast with another group whose heads and necks were protected with steel helmets. She found that even animals whose heads were perfectly immobilized and shielded develop the biological hallmarks of traumatic brain injury: broken-down nerve pathways, swollen brain cells, accelerated cell death, and the buildup of gunk you would expect to see in a brain-tissue sample of an Alzheimer’s patient. The findings suggest that helmets alone may fail to protect the brain from a blast. If true, then combat vests may not only need to deflect the shrapnel from an explosion but also dampen blast-wave frequencies.
How can a blast jump-start brain decay? Cernak theorizes that the rapid compression of organs and tissue in the torso sends a spike of energy rippling through the vessels, including those that loop through the brain. She envisions tiny bursts of pressure that squeeze brain cells and warp the connections between them in ways that are too subtle to show up on standard MRI scans. It’s the cumulative result of stretching nerve endings, she believes, that triggers a domino effect of chemical and molecular changes that damage brain cells and disrupt the normal flow of information. It takes time for these changes to snowball, and she thinks this explains what she calls a “slow cooking” of lab animals’ brain cells that can lead to long-term tissue degeneration. It might also explain why some soldiers’ symptoms never seem to clear up.
School of Hard Knocks
Cernak’s lab is not alone in the search. Among the experiments in Darpa’s program, called PREVENT (for Preventing Violent Explosive Neurologic Trauma), researchers are exposing pigs to live munitions and then analyzing their brain tissue for damage. During the explosions, sensors record the full range of physical characteristics of the blast, including peak pressure, the frequency of the blast wave, the electromagnetic pulse (EMP) generated by the blast, the burst of light, the volume of noise, and even the gases generated.
Geoffrey Ling, who oversees PREVENT, believes that most scientists are focused too narrowly on the effects of blast pressure. He’s not at all convinced that it’s the culprit—or at least not the only one. He points out, for instance, that an electromagnetic pulse could affect electrochemical impulses in the brain, but nobody has studied this possibility. Ling notes that steel helmets worn in World War II and Vietnam reflect EMPs, whereas today’s Kevlar helmets don’t. “A 155-millimeter artillery shell sends out an EMP so strong that it will short-circuit our radios,” he says. “If there is something that could short-circuit an electrical pathway in the brain, that could disrupt function, I really want to rule that out.”
Pig data is telling, but there’s no substitute for a controlled study on humans. One of the most promising is a clinical trial involving breachers. These are the soldiers who blast down doors to storm buildings and, as a result, are guaranteed to get their bells rung on a regular basis. Lee Ann Young, a mechanical engineer who works for Albuquerque defense contractor Applied Research Associates, is studying a group of Marines as they go through breacher school at their base in Quantico, Virginia. Before, during and after their training, they will undergo MRIs and neurobehavioral testing for hearing and balance.
They will be outfitted with pressure gauges to measure the strength of each of up to 40 blasts that they will be exposed to over a two-week period. “They’re very low-level blasts,” Young says. “I’ve been in the room, and it doesn’t feel that much different than the thump of a speaker at a loud rock concert. The question is whether it’s causing some sort of cumulative neurological impairments.”
As more stories like Hussey’s come out, some experts worry about fomenting fear of a mysterious widespread epidemic. Many make comparisons to the controversy over Gulf War syndrome, a much-debated affliction marked by fatigue, headache, dizziness and respiratory disorders. But although numerous questions remain about what Cernak calls blast-induced neurotrauma, she believes that if scientists accept it as a possibility, there is hope that it can be diagnosed and treated, and perhaps even prevented. “It is not a doomed message,” she says. “It is not that you were exposed to a blast, therefore you have a brain injury. But if you don’t do anything, the potentially reversible changes can become irreversible.”
It’s possible that mental exercises such as the ones Hussey practices could improve some cognitive symptoms, given the brain’s marked ability to heal itself. But the best medicine of all, Hussey says, was simply getting medical validation of his problems. “I wanted things to make sense to me,” he says. “My two weeks down in Tampa answered a lot of questions—a lot of it about my own sanity. I was wondering if it was just me. I don’t feel hopeless anymore.”
How Blast Waves Ambush the Brain
It’s not just flying shrapnel and brute force that cause concussions on the battlefield. Pressure waves may also play a role.
Here’s how
An explosion begins with a powerful pulse of hot compressed gas that radiates outward, generating a wave of pressure that can travel up to 1,500 mph. The bigger the bomb, the faster and more forceful the wave. A vacuum of air trails this initial wave, creating a violent suction force that can shear organs.
But little is known about how blast waves damage the brain. Shock waves rattle the head but may also compress the torso, transferring energy to blood vessels. One theory is that the oscillating waves travel through the bloodstream and into the brain, where they twist and kill neurons over time.
Eric Hagerman is a contributing editor for Popular Science. His last article, in March, was about drug-testing sewer systems.
Record numbers of ex-soldiers in UK jails as combat trauma blamed
At least 8,500 former service personnel are in custody - nearly a tenth of the UK prison population. Jamie Doward reports
- Jamie Doward
- The Observer,
- Sunday August 31 2008
- http://www.guardian.co.uk/uk/2008/aug/31/military.prisonsandprobation
'They don't have the right equipment and they're knackered'. Photograph: John Moore/Getty Images
The number of soldiers who end up in prison for violent offences has increased dramatically in the past four years, according to a report that has raised concerns about the mental health of military personnel returning from war zones. Compiled by probation officers, the report estimates that at least 8,500 former soldiers are in custody - 9 per cent of the UK prison population and nearly double the estimate of a previous study by the Home Office in 2004, which put the figure at 5 per cent.
But even the estimate by Napo, the probation trade union, may be on the low side. In a sign that the Ministry of Defence is increasingly aware of the problem, it recently carried out its own assessment in conjunction with the Ministry of Justice and ex-services charities. A pilot study at Dartmoor prison concluded that almost 17 per cent of inmates had been members of the armed forces.
'It is of real concern that thousands of soldiers are in prison and many more are on parole or community service orders,' said Harry Fletcher of Napo. 'In virtually every incidence the former soldier served in either the Gulf or Afghanistan, became involved in excess alcohol or drug-taking, and was subsequently convicted of an offence of violence.'
The Napo report was compiled from more than 70 case studies. Whatever the true figure, it is apparent that soldiers comprise by far the largest occupational group in the prison system. 'It is clearly worrying that a significant proportion of people in the penal system are ex-servicemen and it doesn't say much for the support given to those leaving the military,' said Andrew Neilson of the Howard League for Penal Reform.
'An inability to cope with civilian life, particularly for those who joined the services on leaving school, can certainly lead to offending and see someone swapping one institution for another.'
Often it is those closest to the soldiers who are victims of their violence. The report cites the example of one serviceman who struggled to adapt to civilian life after six years in the army. His relationship with his partner broke down and she stopped him seeing his children because of his heavy drinking. Verbal abuse turned to physical abuse, which led to a jail sentence.
Another soldier ended up in a prison in Humberside for actual bodily harm. According to his probation report, he started drinking heavily after he returned from having served in Bosnia at the age of 19. The soldier said he had not been prepared for what he saw while on peacekeeping duties. For years he could not get the image of people nailed to trees out of his mind.
'The number of soldiers in prison is definitely on the rise,' said Tracey Johnson of Veterans in Prison, which believes there is a link between the intensity of the army's current missions in Iraq and Afghanistan and the number of soldiers currently in jail. 'They're fighting in back-to-back conflicts, coming out and going back again; they haven't got time to recover. There are not enough of them. They don't have the right cover or equipment and they're absolutely knackered.'
The organisation has been inundated with letters from soldiers in prison. In virtually every case it believes that the writers were suffering from post-traumatic stress disorder (PTSD). One father said that before his son was jailed for threatening to shoot another soldier, he had been wetting his bed and in floods of tears because 'he couldn't get Iraq out of his head'.
'He told me they often had to raid buildings where they believed terrorists were hiding,' the man wrote. 'Because he is a big strong lad, he had the heavy machine gun and so had to enter these buildings first and in his words "was shit scared". I told him anybody would be in that situation, but I got the impression he felt it was a sign of weakness.'
David Bradley, 43, developed post-traumatic stress after serving in Northern Ireland. In 2006, he shot his uncle, aunt and two cousins at close range with a pistol he had smuggled into the UK after serving in Bosnia. Several hours later, armed with a nail bomb, a sawn-off shotgun and a pistol with silencer and ammunition, Bradley walked into his local police station in Newcastle and calmly said: 'I have killed four members of my family.'
As the incidence of post-traumatic stress becomes more prevalent there are suspicions that some soldiers will cite combat fatigue as an excuse for their criminal behaviour. 'There are those who say they have it as some sort of amelioration for their actions,' conceded Peter Poole, director of welfare services at the charity Combat Stress.
The Napo report provides some of the most credible evidence to date that stress is a major factor behind the rise in the number of soldiers going to jail. Dozens of clinical psychiatric assessments speak of soldiers suffering from post-traumatic stress when they attack others. Often the disorder is not identified until the soldier enters the prison system.
'Military operations in recent years have placed the armed forces under increased pressures,' said Derek Howard-Budd, head of welfare at the Soldiers, Sailors, Airmen and Families Association. 'Associated issues like PTSD can take a long time before symptoms develop and much longer to be diagnosed.'
Post-traumatic stress has been dubbed 'the hidden wound' - the injury that is never talked about because of the stigma attached to soldiers suffering psychological problems. 'The idea that it is not a "real" condition is inherited from the First World War, where shell-shock among troops was thought to be a sign of weakness,' said Bridget O'Connell, of the mental health charity Mind. 'Now, with a better understanding of the way trauma affects us, this notion is long-since outdated.'
It was not until he was serving life for murder that Tracey Johnson's husband, Jimmy, who was the victim of a bomb attack while serving in the army in Northern Ireland, became aware he had problems. She fears that many more soldiers will end up going the same way. 'Many of them don't even know they've got it,' she said.
Despite heightened concerns about the prevalence of the condition, there are claims that little is being done to assess soldiers' mental health when they return from war zones. What help is available is usually on an ad hoc basis and often available only when they have been incarcerated. Staff at Everthorpe prison in Brough, East Yorkshire, have become so concerned at the lack of support traumatised soldiers receive upon release that they have taken to issuing them with information packs giving details of mental health charities.
Groups such as Combat Stress can be effective, but have limited resources. 'We can only help those who seek help,' Poole said. 'And there are more people than we are equipped to deal with.'
In a statement to The Observer, the MoD said that counselling was available to service personnel at all times, and pointed out that all troops receive briefings before and after deployment to help them recognise the signs of stress.
'We have launched six pilot schemes of community-based veterans' mental health therapists which will be rolled out across the UK,' the MoD said in a statement. 'Veterans can also receive free mental health assessments from a consultant psychiatrist with a military background. This service is also available to veterans in prison.'
But politicians said it was clear that more needs to be done to identify and treat post-traumatic stress at an early stage. The Labour MP John McDonnell, who is secretary of the Justice Unions All Party Group, said it was time for the government to urgently review systems for supporting serving and retired members of the armed services.
Elfyn Llwyd, a Plaid Cymru MP who has become alarmed at the number of his constituents who have served in the armed forces and are now in prison, said that service personnel and their families were being let down. 'If better treatment was available for these servicemen, hundreds, maybe thousands, would not have offended,' he said.
Veterans In Prison draws comparisons with the United States, where soldiers returning from war zones are put through 'decompression courses' where they are assessed by mental health experts before leaving the base.
'Here they just get them altogether in the barracks and ask them who wants to see a shrink,' Johnson said. 'Nobody's going to put their hand up to that