Speculation: Physical Pain Might Not Be Very Bad?

Levan Ramishvili
Today’s post will be short and speculative. It is about pain, suicide, and euthanasia.
A lot of utilitarians believe pain is very bad. This claim is difficult to assess, partly because it’s not always clear what pain is. Within the domain of physical pain, there are a wide range of kinds of pain which may not be strictly comparable. And mental pain is even more diffuse: is shame a kind of mental pain? Is fear? Is anxiety? Why are we calling everything pain?
Here I will very briefly point out two possible reasons to be skeptical of the idea that physical pain is actually a strong moral concern on its own. I am not committed to the idea that physical pain has no moral weight, but I’m not sure that most people actually think physical pain is as bad as utilitarians seem to think it is.
I’m making this argument free because murdering old people by making them feel ashamed is a very bad thing and we should not allow it.
Recently, I wrote about euthanasia, and why widespread euthanasia is likely to become de facto non-optional euthanasia. A lot of people pushed back with the standard boring argument for euthanasia: sure, maybe widespread euthanasia will have some bad consequences in healthcare markets and innovation, but physical suffering is so bad that we should waive our usual do-not-kill norms.
The logical implication here is “when people are in pain, life becomes less preferred vs. death, and so people commit suicide.”
This is an empirical claim we can test pretty easily. Are suicide and physical pain really that closely tied? Is it really physical pain that plausibly motivates euthanasia?
Answer: apparently not. In the U.S., about 9% of people who die via suicide experience chronic pain. Seems high? Not really: about 9% of adults in the U.S. experience chronic pain. So it doesn’t seem like chronic pain is that strongly associated with suicide in the U.S
One clinical study in Denmark finds almost 4x higher suicide attempt rates for pain patients, consistent with an older meta-analysis that found pain patients generally had 2x higher suicide death rates.
So at the population level, pain=/=suicide. But if we select for pain patients, pain=suicide.
However, that meta-analysis also points to reasons to be skeptical pain is actually leading to suicide:
Is it pain, or is it hopelessness about pain? Is it pain, or is it catastrophizing? Is it pain, or the insomnia after pain?
More recent meta-analyses suggest that pain-suicide studies are mostly low quality, and often don’t even report control groups. A meta-analysis which shows >200% increase in suicidality associated with pain found just a >30% increase in actual suicide, and further notes strong evidence of major publication bias. Another systematic review point-blank says “Suicidality is more related to psychosocial factors than physical factors.”
And most strikingly, suicide-attempters actually have appreciably higher pain tolerance than healthy people. High pain tolerance was even more strongly associated with suicidality than high pain was. At the extreme, I looked for studies of people with insensitivity to pain due to various genetic or acquired conditions. The only one I found had just 3 people with congenital insensitivity to pain. But, lo and behold, they engaged in significant self-harm.
So it seems like more pain doesn’t necessarily mean more suicide, and when it does it’s often because of the mental pain attendant on physical pain, rather than the physical pain itself. Purely physical pain doesn’t really seem to have clear suicide implications.
If this is true, then painkillers shouldn’t reduce suicide.
Spoiler: prescribing pain-sufferers painkillers increases suicides.
I couldn’t find a meta-analysis specifically on this topic. Maybe I missed one. But it seems like chronic pain is not as strongly associated with suicide as the (biased) literature suggests, that high pain-tolerance is modestly associated with suicide, and that pharmacological interventions reducing pain don’t decrease and actually increase suicide.
So it really seems like pain doesn’t cause suicide, and it almost seems like lack of pain causes suicide.
Now, note that I am excluding mental pain here. We’re only talking about physical pain. We can also guess that probably poorer countries on the whole have more pain, right? Here’s IHME age-adjusted suicide rates in 1980, 2000, and 2021:



Those maps are not totally uncorrelated with something like maybe our guess at cross-national differences in pain experience… but like, do Mexican people today experience that much less pain than Americans? Are Greenlanders just unendingly suffering unendurable pain?
It seems way likelier to me that major social trends in suicide just aren’t about variance in physical pain. They’re mostly about cultural norms regulating suicide or psychosocial factors. Physical pain probably isn’t actually a super important suicidality risk.
So I am skeptical of the idea that people choose euthanasia because of physical pain, per se.I think people choose euthanasia because they believe their pain is meaningless, or because they believe it is morally bad to be dependent on other people, or because they feel hopeless, or because they feel it’s expected of them. I seriously doubt that the prevalence of euthanasia by condition is even actually well-proxied by physical pain, especially since some of the highest euthanasia rates is for various conditions related to cognitive decline.
And by the way. I actually happen to have on hand data from the NHIS 1997-2018 waves that asked people about their pain AND their emotions, and then I have it linked to National Death Index data, so we know which of the surveyed people died, and how. Of the over 600,000 people surveyed, about 200 did commit suicide over the ensuing sample window.
Here’s suicides per 100,000 people in each age group, broken out by Did/Did not report chronic pain, and Did/Did not report any level of hopelessness.
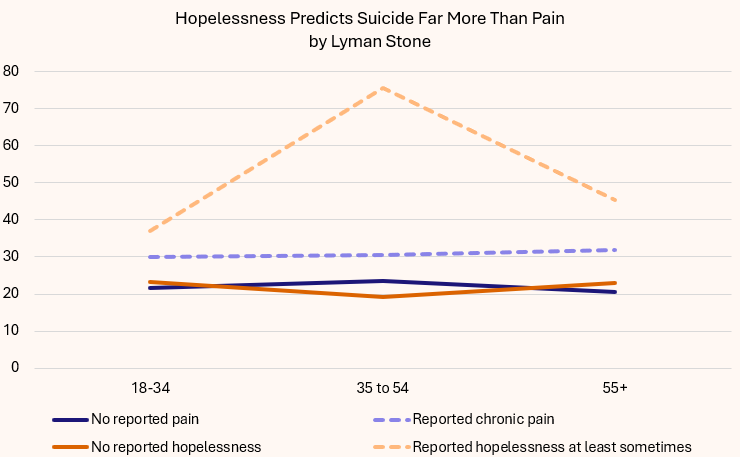
I can tell you, the chronic pain effect is right at the margin of statistical significance. But since we have literally hundreds of thousands of people in this dataset, and lots of them have chronic pain, if chronic pain was gonna clearly cause higher suicide, we’d see a bigger effect.
Kinda like… the effect we see for hopelessness! People who report any level of hopelessness (even just “occasionally”) have much higher suicide rates.
Breaking out by age and specific level of hopelessness means we get very noisy estimates given how rare suicide is, but it sure looks like more hopelessness=more suicide.
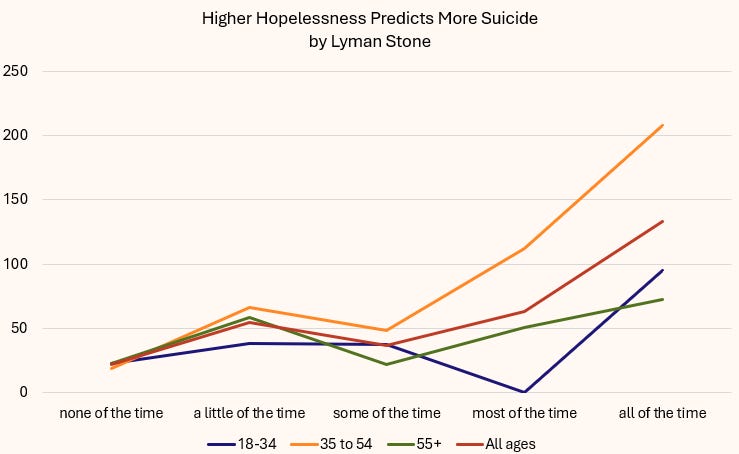
So while physical pain maybe has some very modest effect on suicide at most, emotional and psychological pain is huge. The process by which humans decide life is not worth living anymore is generally not highly connected to physical pain, but rather motivated by the things humans find far more horrifying: loss of self-esteem, dishonor, shame, embarrassment.
Pain Before DishonorHunter-gatherer societies are important to study because they give us a window (albeit an often warped one, since they are not frozen-in-time living fossils) into what life may have been kinda like before agriculture, in the environment where we mostly evolved. I like
‘s work on pain and scarification in foraging societies. A nice synopsis of it can be found just by searching his tweets for “pain.”The takeaway is you will see a bunch of pictures of seriously cut up bodies. Here’s an example from Wikipedia:
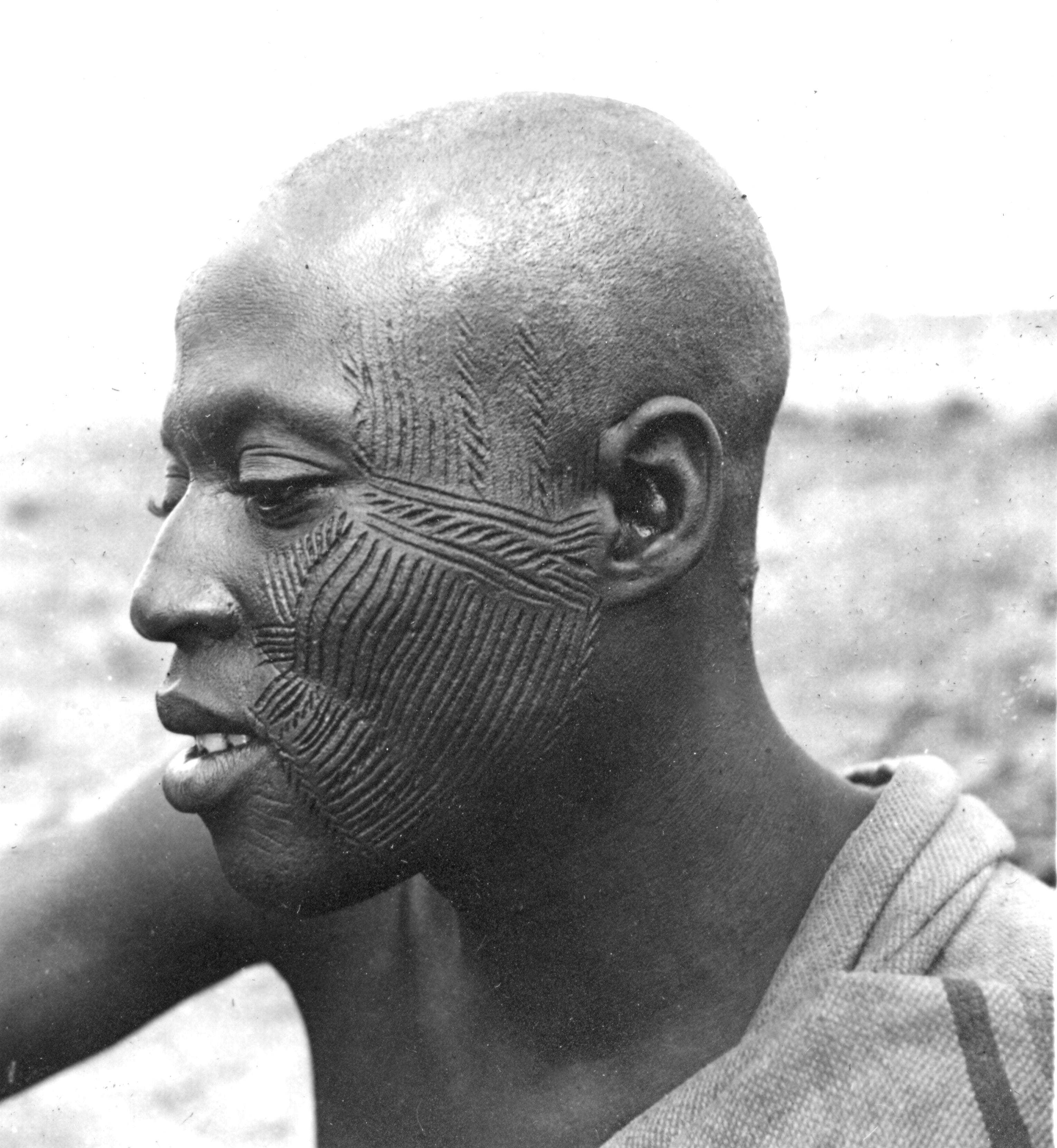
That really hurt. That dude suffered to get that look.
Why did he do it?
The simple reason is honor. He lived in a society where men displayed their manliness, masculinity—status and honor—through resilience to pain. Pain is a widespread part of coming-of-age rituals for young men, and a widespread part of men’s cults which are common in foraging and some pastoralist societies.
We could debate why exactly intentional infliction of pain is so cross-culturally widespread, but on some level it doesn’t matter because we basically know the proximate motivations: status and public honor.
In other words:
Across cultures and even in the environments most similar to our evolutionary ancestral environment, humans will overwhelmingly choose to experience extreme pain rather than dishonor.More broadly, hatred of cowards is pretty cross-culturally widespread. Now, societies may define cowardice quite differently (and
actually has some posts arguing that foragers largely engage in stealth warfare through concealment, not direct fixed piece battles as such), but whatever the local definition of cowardice is, it’s punished pretty severely. Men in particular are expected to not be cowards. They are expected to risk serious pain and even death, and the tool used to motivate this is largely the threat of shame and dishonor. So what do humans hate more than pain and death? Shame and dishonor.When people choose death, it is most plausibly a sign that they feel continuing life is shameful or dishonorable, not that it is merely painful.People do not choose their cultures, for the most part. And regardless, in every culture, honor and shame is about how other people see you. This means that dishonor is always and everywhere inflicted upon the individual. People cannot simply choose to be seen as honorable or dishonorable; they have to take actions prescribed by others whom they wish to impress, in order to obtain honor in their eyes.
In other words, dishonor isn’t consensual. People don’t just get to choose if they have honor or not. Either other people afford it to you, or they don’t. No matter how many times you cry out, “I am a person worthy of honor! I am a person worthy of honor!” if your society doesn’t believe you, you gradually shrink into a corncob and get euthanasia’d. You may sign the paper voluntarily enough, but your honor was taken.
Some cultural norms really are voluntaristic: choices do exist in the world! But if we accept that people basically choose death over life not because of some inevitable fact like physical pain near end of life, but instead because of cultural ideas about hope, honor and dignity as they relate to suffering, dependence as it relates to moral worth, then we realize that a lot of these aren’t strictly optional. People can choose to be hopeful or not, so that one is voluntaristic. You, famously, can’t really steal hope from people as long as they just decide to have it.
But the social status of suffering and the social status of dependence are inherently relational. When they are low-status, sufferers and dependents are rendered low-status, and this is not voluntaristic. It is imposed.
I would argue that the status of suffering is declining. Other moral goods are no longer widely accepted, various kinds of utilitarianism are culturally ascendant, and euthanasia itself is predicated on the notion that suffering has no status.In other words, we are removing the moral and cultural logics which create optionality for sufferers. When suffering is not low-status, people still can choose euthanasia: they won’t be around to suffer the low status arising from their choice to exit early! But when suffering is low-status, the choice is either euthanasia to escape low status, or continuing low status. We already know people very often prefer death to dishonor, so the mechanism of coercion is clear. By creating ever-increasing costs of dishonor, shame, and low status from suffering and dependence, we are creating social norms which effectively will coerce euthanasia.
This is, therefore, a second reason why we should expect that widespread acceptance of euthanasia will lead to coercive euthanasia.
“Well but Lyman…” No that’s wrong too.Clever readers will notice that my argument here implied that physical pain actually isn’t bad enough to justify waiving do-not-kill norms, but that mental pain probably is bad enough, so maybe we should allow euthanasia for mental pain?
But this is a bad argument for two reasons: 1) we’ve already seen how easy it is to abuse mental pain provisions in various horror-show cases in the few places that allow this and 2) if we allow euthanasia for mental pain only then the association between coercive norms and euthanasia would probably be even stronger, and that is the whole bad thing we are trying to avoid here!
“Do I sense a polemic here about animals?” Yes, for sure.The buried lede here is that if physical pain is not as bad as we think it is, and complex mental states are in fact by far the worst kinds of experiences, then our threshold for how much we weight the pain of non-human life forms should be a lot lower than utilitarians suppose. The appropriate standard would be something like brain neurons squared, which would mean that most of the animate biomass on earth has essentially zero moral weight. While some rather simple organisms probably do feel some kinds of emotional horrors beyond physical pain, there is every reason to suppose that the complexity of mental life and the range of awful things which can be experienced rises superlinearly with neurons.
This does establish an extremely compelling argument against killing whales, elephants, large primates, etc, since these creatures by implication would be very morally valuable. It also establishes an argument against any kind of cruelty or indignity for these creatures. The basic argument would be that since physical pain isn’t very weighty, we should create moral weights based on evidence for more cognitively complex kinds of emotional or psychological pain. Animals that don’t pass the mirror test might not even have a sense of self to feel shame about, so we can perhaps say they’re basically morally meaningless. But this is also very weird since one species of ants has passed the mirror test. So I have no idea what to make of that.
Levan Ramishvili
This post is speculative. But I’m writing it now, before the trends I fear come to pass, to lay down a marker. As a note, longtime readers know that I am biased on this issue. I’m a conservative, traditionalist Christian who believes that premature termination of human life solely for the purpose of alleviating suffering is immoral, since the experience of suffering is part of our union with Christ, and the occurrence of suffering is a primary occasion for the virtuous vocations of others. However, I will not lean on those arguments here, though careful readers will notice that my underlying implied view here is that moral virtue is not only virtuous but also imbued into nature in such a way that virtuous norms tend to generate desirable social outcomes, whereas vicious norms tend to generate undesirable social outcomes. Nonetheless, you needn’t accept my moral presuppositions to accept the reasoning below; I note it merely so that you can understand my biases.
A second bias here is that a large share of my income comes from providing research to pharmaceutical companies who are deeply invested in treating, curing, or managing diseases. Widespread choice of palliative care and euthanasia over treatment directly threatens my ability to feed my family, so I have strong economic reasons to prefer that people would continue to choose treat-and-suffer rather than ease-and-die. But again, you needn’t share my economic interests to accept the reasoning below. I simply note it so that you understand that I am not strictly neutral.
I want to make two arguments. First, a counterfactual history; second, a speculative future.
My basic argument will be this:
If euthanasia becomes widespread for specific often-but-not-always lethal conditions, treatment quality and options for those conditions will cease to improve and may rapidly decline.Indulge me in a historical counterfactual. Imagine that it’s 1525 and the Reformation is winding up. Imagine that by some quirk, the Reformers all came to reject the Catholic opposition to abortion, infanticide, and euthanasia. Imagine instead that the Reformers all came to endorse something more like the beliefs of then-rising-in-popularity Edo-period funerary Buddhism, and as a result, Protestant rates of abortion and infanticide rose to 30-50% of conceptions. Virtually all unhealthy children are killed in infancy. At the same time, Protestant doctors invest efforts in treating disabling and nonfatal conditions, but no effort at exploring treatment for foreseeably life-ending conditions. Over the years, Protestants get good at end-of-life pain management, but ultimately popularize euthanasia. By the 1840s widespread access to opium means that pain-free euthanasia is widespread: virtually 100% of forseeable deaths are from euthanasia, perhaps 30% of deaths overall. Over the 19th century as medicine for early deaths improve, more deaths come from causes with drawn-out suffering. By the mid-20th century, 50% of deaths are from euthanasia.
In this scenario, do you think there is as much research effort poured into treating late-in-life causes of death which, when treated, only extend life by a year or two, and QALYs by even less?
To me, the answer is obviously “no.” The herculean efforts the West put into treating these diseases arose from the specific cultural context which made it culturally taboo to just quietly knock off suffering old people. You can’t kill them, you have to treat them. Classic “Hippocratic oath” kind of vibes.
I think that if the West had adopted the value set I describe during its historical scientific development, life expectancy at conception would be ~40% lower today, life expectancy at birth ~25% lower today, life expectancy at age 1 ~10% lower, and life expectancy at age 70 ~10-25% lower.Your exact percentages may vary, but I cannot fathom arguing for 0% lower. And I think the best evidence of this comes from Japan. When Japan began to industrialize after the Meiji restoration, the modernizing government became deeply, seriously convinced that widespread infanticide and the social acceptability of suicide were major obstacles to modern development. As such, they created a special new police force to surveil pregnancy and prevent infanticide: Japan still has one of the most complete systems of pregnancy registration in the world today, and occasionally publishes data from it. In 1873, they also abolished judicial seppuku, and launched a campaign to suppress voluntary suicide.
In the paradigmatic test case of Japan, modernization involved a massive overt change in public norms against infanticide and suicide.To me, that suggests that it really is the case that societies of rapidly improving life expectancy and health are not societies of suicide and infanticide. The cultural norms that induce smart people to invest in finding ways to help old people live incrementally longer or be incrementally more comfortable are not the cultural norms which induce the public to accept widespread suicide as a solution to possibly-terminal suffering.
2. What If Euthanasia Became Genuinely Popular?Now let’s imagine what would happen if euthanasia really became widely popular. The leader in this case is Canada, where maybe 6-7% of deaths involved euthanasia (“Medical Assistance In Dying” or “MAID”). That doesn’t seem super high.
But here it is by major cause group:
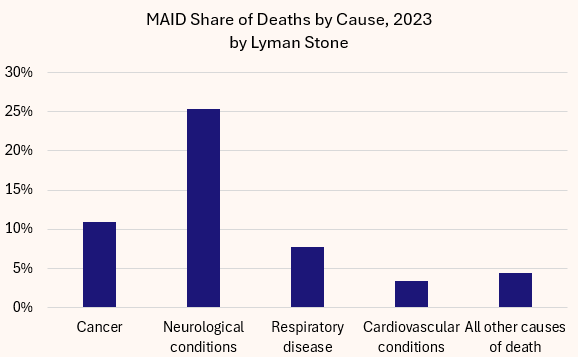
On hand I didn’t see more detailed cause breakouts, so this is what we’ve got. But the key point is this: solidly a quarter of neurologically-related deaths in Canada are already actually people who died when a nurse or doctor injected them with lethal chemicals at their request, and over 1-in-10 cancer deaths.
Imagine you have a rare and dangerous cancer. You are 56. The typical person with this cancer is 67, and their prognosis is bad, maybe 75% mortality within a year. But for you, at your age, it’s more like 40% mortality within a year. But 80% of people with this condition have less than a year to live.
Now imagine two different scenarios. In scenario 1, 75% of the people with <1 year to live pursue palliative care and then euthanasia instead of uncomfortable treatment with low success odds. In scenario 2, 10% choose that option.
Here’s my math:

The key takeaway is “What share of people who get this condition pursue the uncomfortable-but-possibly-lifesaving treatment for it?”
In the high-euthanasia share, just 38% do. In the low-euthanasia share, 91% do.
Now that’s in partial equilibrium.
Now imagine general equilibrium:
How many specialists in this treatment exist when 91% of diagnosed cases pursue treatment? And how many when just 38% of cases pursue treatment?
The obvious answer is that when few people pursue treatment for a disease, fewer doctors specialize in it, fewer researchers innovate in it, etc, etc. Diseases attract specialists and innovation for many idiosyncratic reasons, but the central issue is always going to be “There are lots of patients who want to get a treatment.”
For diseases where a “treatment” only usually means a few more months or years of life after an already long life, and where a “treatment” is almost always a choice to have some amount of short-term additional suffering, the availability and normativity of euthanasia will reduce demand for treatment and thus reduce treatment options.This may seem like a very niche kind of disease, but it actually describes tons of diseases, most especially cancers, but also many neurological conditions.
These are conditions where we should want patients smashing down the doors demanding medical innovation, because these conditions are the current “hard limits” on human longevity. Widespread euthanasia will erode that demand.
The upshot is when an unusually young or good-prognosis person gets the disease, they will have a much harder time finding specialists, and have fewer innovative treatment options.
Seriously, ask somebody who has a really rare disease how easy it is to get treatment and specialist care. It’s incredibly hard. You end up flying around the country for doctor’s appointments. It sucks. Making specialist care more widely available for a given condition boosts survival from that condition.
Thus, widespread condition-specific euthanasia may actually worsen the prognosis for that condition.Point blank, my argument is that euthanasia threatens to undermine the incentive structure driving a lot of medical advancement and innovation, and as such undermine actual health, and perhaps then drive even more euthanasia. It’s not hard to imagine some rarer conditions reaching nearly-100% euthanasia rates.
And so, coercionCoercion is a tricky word and people debate what it means. But here I mean just “you won’t have options.”
If you get a condition where everybody else with it chooses euthanasia, you eventually won’t have a lot of other care options.Doctors won’t have experience treating you. Drug companies won’t produce the medicines that might save you. If clinical trials happen at all, they won’t proceed to commercial stages.
I have a dear friend whose child has a severe genetic condition; they entered a trial for a somatic gene-editing drug. The drug worked, cured the condition. The kid’s life expectancy rose from <10 years to >60 years from one drug with no continuing need for medication. The trial worked perfectly. The drug, however, will never reach the marketplace because the condition is too rare, the drug too costly and experimental, and so it won’t be viable to market the drug.
Beyond lack of options, if 90% of patients choose euthanasia, medical staff and insurers will almost certainly nudge, cajole, badger, and pressure patients to take that route. Treatment will be treated as nonstandard, requiring justification, etc, etc.
None of this will be conspiratorial. There won’t be death panels killing off olds. Your doctor isn’t gonna wait until you’re not looking and jab you with murder juice. It will all be perfectly normal, hygienic, medical. Consent forms will be signed. Due diligence will be conducted having verified that there were no reasonable treatment options. But the reason there were no reasonable treatment options will be that before you ever got sick, other people choose euthanasia over suffering, and as a result, you will preventably die earlier and without even an option of fighting.