Building a Better Mortality Prediction Rule
Aug 22, 2014 08:00 am | Christian Sinclair
You will often hear the lament from people within and outside of the hospice and palliative care fields, that doctors are pretty bad at making effective prognostication. Patients and families frequently search for a predictable road map to understand the course they are likely on, and even when they cede the understandable uncertainty to the physician, the doctors will often reply with an unhelpful retorts like, “I don’t know what may happen. There is only one person who does.”
I doubt all of those physicians are referring to Dr. Mark Cowen, but they may want to take notice of what he and his colleagues at St. Joseph Mercy Hospital in Ann Arbor, Michigan have been doing for the past couple of years. Having already developed and validated a 30-day mortality prediction rule (MPR) (published in 2013), the team now advanced the idea to a prospective, real-time mortality prediction rule study. Published online in the Journal of Hospital Medicine this month, “Implementation of a Mortality Prediction Rule for Real-Time Decision making: Feasibility and Validity” may help clinicians move from pre-contemplation to contemplation when it comes to applicable prognostication.
The MPR in this study was completed on almost 10,000 patients admitted to the hospital (78%) and an outpatient surgery center (22%) at a tertiary community teaching hospital over the Fall 2012 to Winter 2013 (yup, flu season!). Some high mortality risk (dialysis units, transfers from outside hospitals) and low mortality risk admissions (child birth/OB) were not included, most likely because the ability to implement the rule before having a bed assigned was more challenging to accomplish. Since this is not only a validity study, but also a feasibility study, they nicely discuss the diplomacy, champion-finding, and need for paid support staff for this project to work. Interestingly, the authors note the ED staff were open to this prediction rule only if they could accomplish the task “within the time a physician could hold his/her breath.” Be careful what you say in a research administrative meeting, you may see those words published in a journal article some day!
The rule was Web-based and pre-populated data from the EMR without any manual effort. Updates were done to the Web-based rule as often as every minute! Then ED doctors or surgery center nurses reviewed the pre-populated information and made overrides if necessary. Samples of the questions asked include:
History or presence on admission of:
- Atrial fibrillation
- Solid-tumor cancer
- Metastatic cancer
- Cognitive deficit
- Leukolymphoma
- Other neuro deficit
Patient’s current condition/treatments:
- Respiratory failure
- Heart failure Injury
- Sepsis
- Abnormal vital signs
 At first the clinicians did not have access to the score but that changed over the course of the study, which to me is one of the weaker parts of the study. It treats this whole group as one, but really this is equivalent to having a study where you have blinded the clinicians and the patient, and then midway through you started to un-blind some of them as to the treatment/test/intervention. The authors talk about two care processes put in place as these scores became available which may impact the true validity of this MPR de novo. Wouldn't it make more sense to test this MPR without changing any behavior (via knowing the score), and then test how it could impact clinical delivery and patient outcomes? The impact of this MPR was a slight bit muddled because of that contamination of the study population. At first the clinicians did not have access to the score but that changed over the course of the study, which to me is one of the weaker parts of the study. It treats this whole group as one, but really this is equivalent to having a study where you have blinded the clinicians and the patient, and then midway through you started to un-blind some of them as to the treatment/test/intervention. The authors talk about two care processes put in place as these scores became available which may impact the true validity of this MPR de novo. Wouldn't it make more sense to test this MPR without changing any behavior (via knowing the score), and then test how it could impact clinical delivery and patient outcomes? The impact of this MPR was a slight bit muddled because of that contamination of the study population.
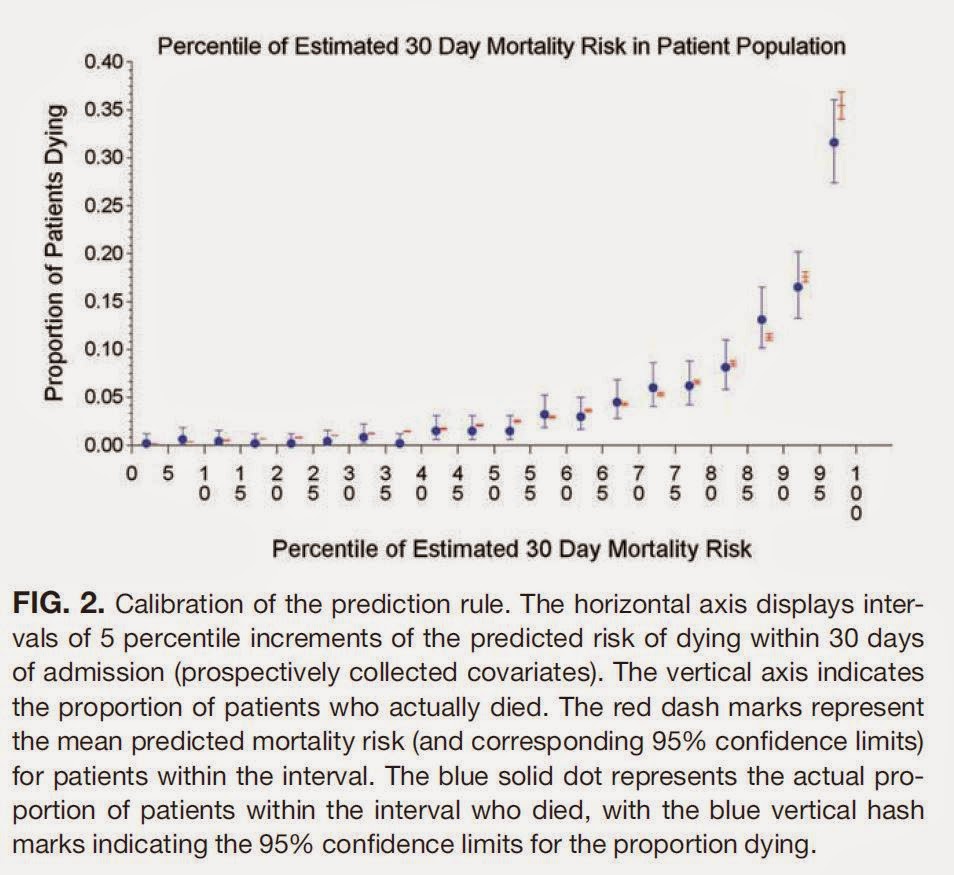
They split the population into 5 risk categories by quintiles, with the highest risk population having an approximate 7-35% chance of 30d mortality.
But let’s get to the real meat of what Pallimed readers care about, did this study group look at palliative care consults, or hospice utilization? Sorta, kinda. We're going to need to do a little hypothesizing and I will expand on that in an upcoming post. We will talk about what an accurate MPR could do for palliative care and hospice utilization.
Of note, nurses worked with this tool, so if anyone says that prognostication is not the role of a nurse, you can point them to this article. Nurses should not be excluded from prognostication based on credentials. I appreciate when nurses give me an honest assessment of prognosis, and I hope other doctors out there do as well.
Some other information that would be really helpful is understanding the outliers in the high risk strata. Who were the people who lived but were high risk? And for how long? Do they have any significant quality of life issues post-hospitalization?
Other info that would be great to see is how much overlap there was in the different groups. For example, if you had palliative care while in the hospital, what was your likelihood of a 30d readmission.
So overall, this is a really good study, and is very accessible in the way it is written. Since it is published in a non-core HPM journal it should be quite easy to approach your hospitalists and ED colleagues to talk about possibly doing a validation study in your local hospitals.
Credits: Future Road Sign - iStockPhotos; Quote - Illustration by Pallimed; Chart - From article under Fair Use guidelines for for nonprofit educational purposes. Full copyright of that figure is retained by the journal.
 Cowen, M., Czerwinski, J., Posa, P., Van Hoek, E., Mattimore, J., Halasyamani, L., & Strawderman, R. (2014). Implementation of a mortality prediction rule for real-time decision making: Feasibility and validity Journal of Hospital Medicine, Early Publication DOI: 10.1002/jhm.2250 Cowen, M., Czerwinski, J., Posa, P., Van Hoek, E., Mattimore, J., Halasyamani, L., & Strawderman, R. (2014). Implementation of a mortality prediction rule for real-time decision making: Feasibility and validity Journal of Hospital Medicine, Early Publication DOI: 10.1002/jhm.2250 |





