AP1189 a Erk1/2 pathway without Mcr1 or Mcr3 activation, I do not see as a commercial threat to afamelanotide. Hruby patent for Mcr3 selectivity has gone nowhere.

Uhohinc
Uhohinc

Claes Svensson
Uhohinc
Uhohinc
WIPO (PCT)
Other languagesFrenchInventorTorbjörn LundstedtAnna SkottnerArne BomanPer AnderssonElisabeth SeifertVictor AndrianovUhohinc
Uhohinc
Claes Svensson
These guys running SynAct Pharma has taken quite a few substances through clinical phases and done some deals with Big Pharma such as Abbvie, Pfizer, Questcor etc. I think they know what they are doing.
Claes Svensson
Uhohinc
Claes Svensson
Just recently this was announced:
“The project is a natural next step in our long-standing collaboration with Dr Trini-Montero Melendez and Professor Mauro Perretti. Our investment of ~£400,000 is to enable an important task of the project, i.e. to link clinical outcome of treatment with our AP1189 compound to MCR1 polymorphism as it would give the possibility to apply a rational approach for patient selection for future clinical studies. In addition, new insight into pharmacology of specific MCR1 variants can be used for identification of next generation compounds”, says Thomas Jonassen, CSO SynAct Pharma."
Uhohinc
Uhohinc
Claes Svensson
All through that text - COMPOUNDS. Nothing is secret, but you probably suck at Google. The melanocortin-system is not fully understood, and therefore all of the action of AP1189 can not be understood.
Uhohinc
Uhohinc
All through that text - COMPOUNDS. Nothing is secret, but you probably suck at Google. The melanocortin-system is not fully understood, and therefore all of the action of AP1189 can not be understood.
Uhohinc
Uhohinc
Claes Svensson
https://synactpharma.com/en/synact-pharma-initiates-resovir-scientific-and-clinical-collaboration-to-explore-ap1189-in-viral-infections/
The brazilian trial is named "EFEITOS DA ADMINISTRAÇÃO DO AP1189, UM ATIVADOR DE VIAS PRO-RESOLUTIVAS, NAS ALTERAÇÕES PULMONARES DE PACIENTES COM COVID-19 E OXIGENAÇÃO COMPROMETIDA (RESOLVIR)"
THE PROJECT, is a new collaboration announced 2 weeks ago, and is about personalized medicine. Every person has a different set of genes making up their MC-receptors. AP1189 will bind better to some patients, and less to others. This is a study to find the different gene-types, and then by a simple blood sample be able to tell beforehand if the patient will be a responder or not. Not everyone responds to melanocortin treatment.
Like, why even highlight "sold their lead candidate to AbbVie"?
Uhohinc
Claes Svensson
"by a Doctor in the Amazon wading thru sewage" - yup... https://scholar.google.com/citations?user=njJyXhsAAAAJ&hl=en
Binding of melanotropic hormones to the melanocortin receptor MC1R on human melanocytes stimulates proliferation and melanogenesis:
https://pubmed.ncbi.nlm.nih.gov/8612494/
Uhohinc
Yesterday, preliminary data from SynAct Pharma’s Phase II study with the drug candidate AP1189 in patients with rheumatoid arthritis was released. The data indicate that AP1189, administered in doses of 50 mg, is safe and well-tolerated. The blinded review of the data also indicates a substantial reduction in disease severity among two thirds of the patients, which may be attributed to AP1189. BioStock reached out to the company’s CEO Jeppe Øvlesen for a comment on the positive indicative results.
When you read about Ap1189 about the goal is it is really only an "add on treatment" to be used with other drugs.......................Aspirin is an anti inflammatory and will get better efficacy results than this drug did in its own trial. Numerous anti inflammatory on market are already getting better results with no adverse effects........If AP1189 works, lets see it without the need to pair it to other known to work in extents drugs for RA.
the below excerpt, is gobbleydeegook double speak for 50mg did not show efficacy, so they intend to use 100mg and make you think it is intentional.....with an oppurtunity to show efficacy..............why not do that from the start..........you do not need another safety profile, that was phase I
Excerpted from below fake interview from SynActin.........................." In the short-term this means that we can focus on getting a safety profile on the next dose level of 100 mg and, if this dose, which was very well-tolerated in our Phase I study, turns out to be safe in the patients as well, we can continue in the second part of the study with two doses of active compound vs placebo. That gives us a great opportunity to show efficacy and thereby confirm the potential of AP1189 as new treatment option in rheumatoid arthritis."
Make sense of this, all I can figure is they are preparing to hide the patients that do not report the way SynActin finds positive......................................wthf.................a rigged trial result.....
"you state that it is unlikely that all patients in the planned 100 mg cohort in part 1 of the study will be registered, dosed and reported "
SynActs pipeline. Click to enlarge
SynAct Pharma´s leading drug candidate AP1189 is a First-in-Class melanocortin receptor agonist targeted at active inflammatory and autoimmune diseases. The primary indications for AP1189 are active rheumatoid arthritis (RA) and Nephrotic Syndrome (NS), but recently the Danish biotech added AP1189 as an adjunctive therapy in hospitalised patients with Covid-19 infection in order to prevent ARDS, to it’s pipeline, given the common denominator in all three indications; an uncontrollable inflammatory response.
Based on the endogenous hormone melanocortin
SynAct Pharma’s research platform is based on the endogenous hormone melanocortin, which is activated in inflammatory conditions and contributes with anti-inflammatory effects that are crucial for the healing process and recovery to normal tissue function.
The treatment concept is based on strengthening the immune system’s healing mechanisms by activating the body’s own immune cells, a so-called resolution therapy. By activating the body’s immune cells, SynAct Pharma´s concept differs from biological and immunosuppressive drugs, which act by inhibiting the activity of the immune system.
Rheumatoid arthritis (RA)
Rheumatoid arthritis (RA) is a chronic inflammatory disorder, which means that the immune system mistakenly attacks healthy cells in the body, causing inflammation and painful swelling in the affected parts of the body. RA affects not only the joints in hands, wrists, and knees, for but also organs like the skin, eyes, lungs, heart, as well as blood vessels. The tissue damage can cause long-lasting or chronic pain, unsteadiness and deformity. Thus, the disease is associated with progressive disability, premature death, and hence, also socioeconomic burdens.
While new types of medications have improved treatment options dramatically, severe RA can still cause physical disabilities. It is in this space where SynAct Pharma wants to position its leading candidate AP1189, with its potential to induce disease remission without concomitant immune-suppression and thereby increased risk for infections, both in RA and other inflammatory and auto-immune diseases.
An early add-on treatment in RA
In the ongoing study, AP1189 or placebo is dosed once daily in previously methotrexate (MTX)-naïve patients. Methotrexate, a chemotherapy agent and immune system suppressant, is one of the most effective medications to treat RA on the market.
Still, approximately 40% of the patients have an inadequate response, while next-line treatments are more efficacious, but often have severe side effects. Even with expensive injectable biologics, up to 30% still suffer from inadequate treatment.
SynAct Pharma´s strategy is to position AP1189 in this context as an early “add-on” treatment that could reduce the need for second-line treatment and/or reduce the dose levels of MTX.
New phase II data in RA
Yesterday, SynAct Pharma announced that the first of two tested doses (50 mg) with AP1189 in early RA patients with active joint disease, was safe and well-tolerated, based on a blinded review of data from the company’s ongoing placebo-controlled Phase II study, which, to date, has enrolled 12 dosed patients from sites in Denmark and Sweden.
The results also show a strong 50% reduction in disease severity in 8 of the 12 patients tested. However, since the review of the data was blinded in order to avoid inserting bias into the analysis, it remains inconclusive whether the reduction in disease severity can be attributed to AP1189.
Based on these results from the double-blind study of the safety, tolerability and efficacy of AP1189, the company has decided to proceed with dosing at the next dose level (100 mg) in part 1 of the study, and to include the 50 mg dose level in part 2 of the study. It will later determine whether 100 mg is safe and tolerable and whether the dose should be included in part 2.
BioStock reached out to SynAct Pharmas CEO Jeppe Øvlesen for a comment on the released data in RA.
Jeppe Øvlesen, to begin with, the preliminary results based on the blinded data, show that administration of AP1189 seems to be safe and well-tolerated. Thus, you have achieved an important milestone in your RA project. What significance does this have for the future development of the candidate?
– For us, it is extremely encouraging to see that, according to the data, the treatment setup and the dose of the compound given to patients is safe. The interpretation on the blinded data on efficacy further support that we should continue dosing at this level in the second part of study.
– In the short-term this means that we can focus on getting a safety profile on the next dose level of 100 mg and, if this dose, which was very well-tolerated in our Phase I study, turns out to be safe in the patients as well, we can continue in the second part of the study with two doses of active compound vs placebo. That gives us a great opportunity to show efficacy and thereby confirm the potential of AP1189 as new treatment option in rheumatoid arthritis.
Going into the numbers, after a 4 week treatment period, a group of 8 patients showed a reduced clinical disease activity index (CDAI) score compared to pre-treatment levels with a median reduction of 50%, and a group of 4 patients with a worsening in their clinical status, where the median CDAI score was increased by 10%. The numbers – considering that it is the common understanding that it takes several weeks before MTX induces improvement in symptoms – sound indicative of a substantial clinical improvement, is that how you would interpret them?
– I have to emphasize that the data is blinded, the sample size is small and there could placebo treated among the subjects where we have identified a fall in clinical disease score. Saying that there is as we highlight in the PR patients that goes from high disease activity to low disease activity within the study period. Such reductions in disease activity are very seldom seen following 4 weeks treatment with MTX as monotherapy. However, we cannot exclude an extraordinary placebo effect. We have to wait to make any conclusions until we have the planned patients enrolled and unblind the data.
Considering the review of the data was blinded, it cannot be ruled out that there are placebo-treated patients among those showing clinical improvement. How does this caveat play into choosing the next dose level?
– The decision to go to the next dose level is based on the safety review not on blinded review of potential efficacy. We could have had a setting where most of the patients still had high disease activity at the end of the treatment period – which the data shows us we are not.
You plan to position AP1189 as an additional treatment given early to patients with RA, in combination with methotrexate (MTX). What reactions and support have you received from major pharmaceutical companies and researchers when presenting this new combination strategy?
– The setup is in many ways ambitious as we go in early start dosing in parallel with methotrexate in patients with high disease activity. In these patients the physician often turns to intraarticular injections of glucocorticoids to induce pain relief in parallel with up-titration of methotrexate as the onset of clinical effect of methotrexate is slow. If the treatment profile of AP1189 in combination with Methotrexate turns out to be effective it could reduce the need for glucocorticoid injections and potentially reduce the need for second-line treatments like biologics or JAK inhibitors.
– If that turns out to be the case, the physicians would find AP1189 as a very attractive opportunity, also because the compound seems not to induce immunosuppression. The pharma industry would likewise see a big opportunity in such a scenario – where it would also serve as part of proof of our “resolution therapy treatment”.
In the press release yesterday, you state that it is unlikely that all patients in the planned 100 mg cohort in part 1 of the study will be registered, dosed and reported during the second quarter of 2020. This seems to have made the market somewhat ambivalent when looking at the relatively small increase in the share price. Would you like to comment on how your chances of success are affected by the Covid-19 outbreak?
– The Covid-19 outbreak has, until further put the recruitment in Sweden and Norway on hold. In Denmark recruitment continued but at a lower recruitment rate. However, we now slowly see that the countries get better control with the corona situation and we hope we will get back to a more normal situation. This will help us in getting the recruitment rate up again and making it possible to get the patients for both the first and the second part of the study enrolled.
Finally, what milestones can we look forward to during the rest of the year?
– We still have the ambition for significant progress in the RA study. We expect to get the study in nephrotic syndrome up and running and then we have the opportunity in Covid-19 where we are working on the protocol and where we have had very good progress with the investigators.
The content of BioStock’s news and analyses is independent but the work of BioStock is to a certain degree financed by life science companies. The above article concerns a company from which BioStock has received financing.
Prenumerera på BioStocks nyhetsbrevUhohinc

macgyver
Uhohinc
Uhohinc

Vallaurix_CUV
 .
.Claes Svensson
" RArthitis trial phase II had 12 patients on the drug................thats all"... You told me you could read?
So the RA-study only has 12 patients? Only a retard would think that after looking into the facts. The study is to screen up to 135 patients, estimated inclusion between 90-115 patients.
Aspirin? Against severe rheumatoid arthritis? Come on, theres gotta be some limit of your stupidity. Severe RA is treated with MTX/DMARDS, biologics, JAK-inhibitors etc... Aspirin? Wow...
"which may be attributed to AP1189" - for obvious reasons dumbass, its a double blind study. But some patients have reached 80% decrease in CDAI-score. Cant give credit to either MTX or placebo on that one buddy.
The management and board owns +20% of the shares, in lockup since IPO in 2016, and the lockup-period goes all through 2021 and over the 3 study results.
Uhohinc
Uhohinc
macgyver
Claes Svensson
And once again I will have to set the facts straight and show the world what a lying little cunt you are :)
You really think that I'm here for your opinion? HAHAHA! You? I know more than you ever will on this subject :)
https://synactpharma.com/en/synact-pharma-expands-ap1189-begin-study-in-rheumatoid-arthritis-uk-version/ Data's so strong that expanding from 90 to ~105 patients will show STATISTICAL SIGNIFICANCE, and not just only Proof of Concept.
The independent DATA SAFETY MONITORING BOARD said "OK GO" for 100mg after first 12pat was dosed on 50mg - and the interim included 26 patients and both dosages.
https://synactpharma.com/en/synact-pharma-announces-positive-interim-phase-2-data-of-ap1189-in-rheumatoid-arthritis/
Uhohinc replies -"BUt tHIS Is NOt tHe AMeriCaN WaY, ThaT cAnt Be GoOd - I KnoW EveRYtHIng"
SynAct Pharma AB (“SynAct Pharma”) hereby announces that the company together with Prof Mauro Teixeira, MD, PhD, Universidade Federal de Minas, Belo Horizonte, Brazil and Prof Mauro Perretti, PhD William Heavy Research Institute, Barts and the London School of Medicine, Queen Mary University, London, UK has established a scientific and clinical collaboration, RESOVIR (resolution in viral inflammation), aimed to investigate pharmacological promotion of inflammatory resolution as a novel approach to control viral infections. The first step of the collaboration will be to run an exploratory clinical study in Covid-19 infected patients aimed to investigate repeated dosing of SynAct Pharma´s clinical stage compound AP1189. Later the collaboration will investigate the potential of promoting inflammatory resolution in other viral diseases such as Dengue and Influenza virus."
SynAct will have the rights for the combination treatment in RA with Ap1189+MTX till 2041.
Patent for treating ARDS with AP1189 was applied on April 3, 2020. So patent is on the way. Takes ~18 months before application is published and searchable in databases.
Looks like someone (you) is desperately is looking for confirmation bias. Twisting the facts to match your opinion etc...
Uhohinc
Uhohinc
Claes Svensson
You americans can't even invest in SynAct Pharma haha, so that would be alot of time wasted. I came here because you had no idea what you were talking about. You described AP1189 totally wrong, thats all you stupid fuck.
Haha, the neverending story of lies, so now the annual meeting with standard protocols in accordance with swedish laws are fishy?
Uhohinc
Uhohinc
You americans can't even invest in SynAct Pharma haha, so that would be alot of time wasted. I came here because you had no idea what you were talking about. You described AP1189 totally wrong, thats all you stupid fuck.
Haha, the neverending story of lies, so now the annual meeting with standard protocols in accordance with swedish laws are fishy?
And once again I will have to set the facts straight and show the world what a lying little cunt you are :)
You really think that I'm here for your opinion? HAHAHA! You? I know more than you ever will on this subject :)
Just recently this was announced:
Uhohinc
T.E.N.J. is shareholder in SynAct Pharma and owns intellectual property on AP1189.
Uhohinc
Uhohinc
SynAct Pharma AB (“SynAct”) today announced that the first subject has been dosed in a clinical study in healthy volunteers to describe the pharmacokinetics of AP1189 following administration of a new tablet formulation aimed for once daily dosing in further clinical development of the compound.
The study is a single center, open label, 3-part pharmacokinetic study, with 12 healthy subjects in each part. The primary objective of the first part is to determine the relative bioavailability of AP1189 after dosing with the newly developed tablets versus the oral suspension used so far in clinical trials.
In the second and third part of the study, the food effect on the pharmacokinetics, which is a regulatory requirement, and proportionality following dosing at different dose levels will be evaluated.
“This is a crucial step in the development of AP1189. We are eager to see the results of dosing AP1189 as tablets to humans. We have succeeded in making AP1189 tablets that meet our expectations. Importantly, the manufacturing process allow for further development, including scaling as will be required for clinical development in later phases.”, said Thomas Boesen, COO, SynAct Pharma.
Preclinical testing of the tablets supports that the pharmacokinetic profile of AP1189 in plasma is comparable or better after dosing of tablets than after dosing of the suspension currently used in the phase 2a clinical development, and when confirmed in humans, the tablets will be used instead of the suspension in future clinical trials.
“The new tablets will enable supply of AP1189 to a wider population of patients, with the aim to enhance safety and compliance. The new formulation shows unique characteristics with regard to compound release that has been covered in the IP application we filed in June and will give an additional level of protection on the AP1189 product once granted.”, said Thomas Jonassen, CSO.
The information was submitted, through the agency of the contact person below, for publication on October 15, 2021
For further information aboutSynActPharma AB, please contact:
Jeppe Øvlesen Thomas Jonassen
CEO, SynAct Pharma AB CSO, SynAct Pharma AB
Phone: +45 28 44 75 67 Phone: +45 40 15 66 69
Mail: j...@synactpharma.com Mail: t...@synactpharma.com
AboutSynActPharma AB
SynAct Pharma AB conducts research and development in inflammatory diseases. The company has a platform technology based on a new class of drug candidates aimed at acute deterioration in chronic inflammatory diseases with the primary purpose of stimulating natural healing mechanisms. For more information: www.synactpharma.com.
About AP1189
The mechanism of action of SynAct Pharma ́s lead compound AP1189 is to promote resolution of inflammation through melanocortin receptor activation directly on macrophages, thereby reducing the pro-inflammatory activity of macrophages and by stimulating macrophage efferocytosis, a specific ability to clear inflammatory cells (J Immun 2015, 194:3381-3388). This effect has shown to be effective in disease models of inflammatory and autoimmune diseases and the clinical potential of the approach is currently tested in two clinical phase 2a studies in patients with active rheumatoid arthritis and in nephrotic syndrome.
https://clinicaltrials.gov/ct2/show/NCT04004429?term=AP1189&draw=2&rank=1)
https://clinicaltrials.gov/ct2/show/NCT04456816?term=AP1189&draw=2&rank=2
Jeppe Øvlesen Thomas Jonassen
CEO, SynAct Pharma AB CSO, SynAct Pharma AB
Phone: +45 28 44 75 67 Phone: +45 40 15 66 69
Mail: j...@synactpharma.com Mail: t...@synactpharma.com
SynAct Pharma AB conducts research and development in inflammatory diseases. The company has a platform technology based on a new class of drug candidates aimed at acute deterioration in chronic inflammatory diseases with the primary purpose of stimulating natural healing mechanisms. For more information: www.synactpharma.com.
Tags:
Uhohinc
SynAct’s drug candidate, resomelagon (AP1189), is a once-daily oral selective melanocortin agonist. resomelagon (AP1189) selectively stimulates the melanocortin receptors that are directly involved in inflammation and its resolution without stimulating the adrenal glands to release cortisol. This selectivity enables resomelagon (AP1189) to exert its anti-inflammatory and immune resolution effects in a steroid-free manner without the significant safety, tolerability, and side effect issues associated with adrenocorticotropic hormone (ACTH) based therapies. Resomelagon (AP1189) is also a biased agonist that does not stimulate melanocortin pathways that are responsible for off-target activity like skin hyperpigmentation.
The company is evaluating resomelagon (AP1189) in three Phase 2 clinical programs: rheumatoid arthritis (RA), idiopathic membranous nephropathy (iMN), a form of nephrotic syndrome, and virus-induced respiratory insufficiency (VIRI) like that seen in COVID-19. In 2021, SynAct successfully completed Phase 2a trials in early severe RA and in hospitalized patients with COVID-19-induced respiratory insufficiency. Also in 2021, SynAct successfully tested a new oral solid tablet formulation of resomelagon (AP1189) in healthy volunteers and filed additional composition patents that should provide molecule exclusivity past 2040.
In 2022, the Company initiated two new Phase 2 clinical trials in RA: EXPAND a Phase 2b trial in newly diagnosed RA patients experiencing severe disease activity and RESOLVE a Phase 2a/b trial in RA patients experiencing an incomplete or loss of response to methotrexate. In addition, the ongoing Phase 2a iMN trial was amended in 2022 to introduce the new oral tablet dosage form and to increase the treatment period to 3 months. Topline results from all three studies are expected in the second half of 2023.
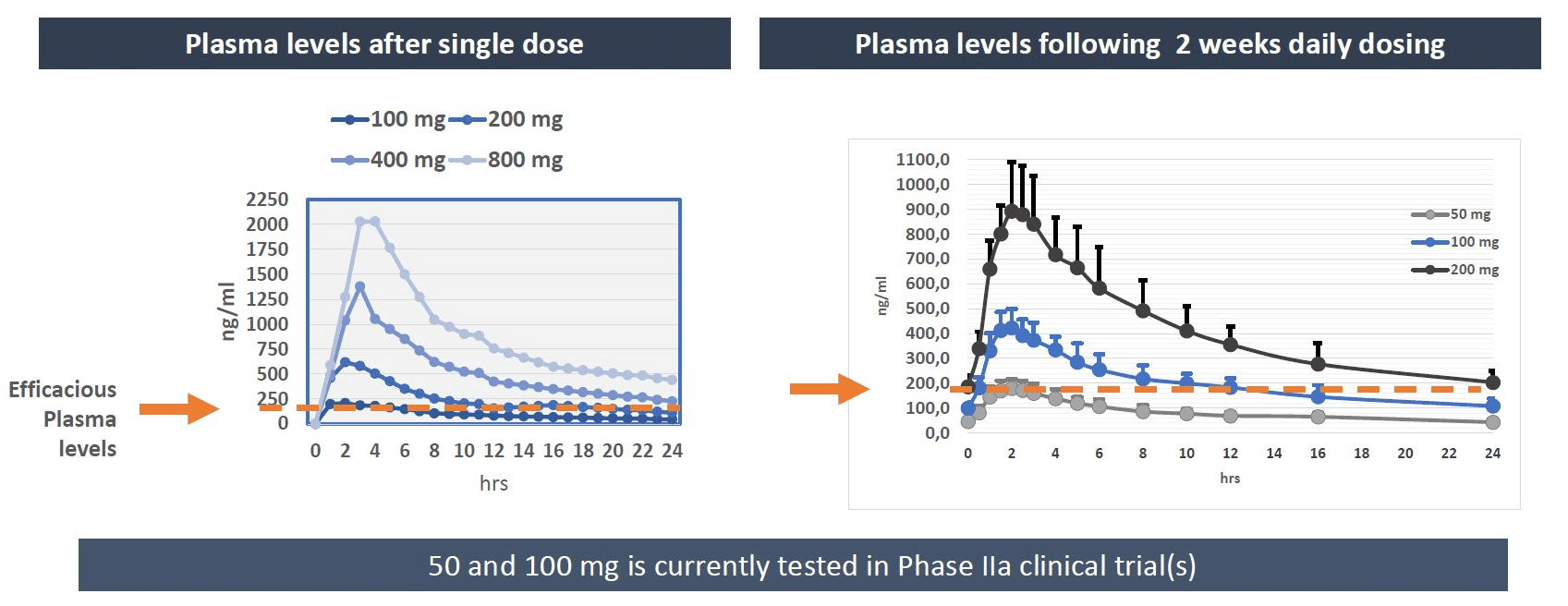
Phase 1 DevelopmentIn the Phase 1 clinical assessment, 2 weeks of once-daily dosing of resomelagon (AP1189) supported continued development as a once-daily orally dosed medication. The plasma concentration needed induce pharmacological efficacy was reached within 1.5 hours of dosing and daily exposure is increased until steady state has been reached following 5-6 days of treatment after which no further drug accumulation was observed.
Importantly, no treatment limiting adverse events were identified following multiple dosing and doses used in the ongoing Phase 2a studies (50 and 100 mg) were found to be safe and well tolerated.
SynAct Pharma is a clinical stage biotechnology company focused on resolving inflammation with melanocortin biology. Selective activation of the melanocortin system can help the immune system resolve excessive or chronic inflammation.